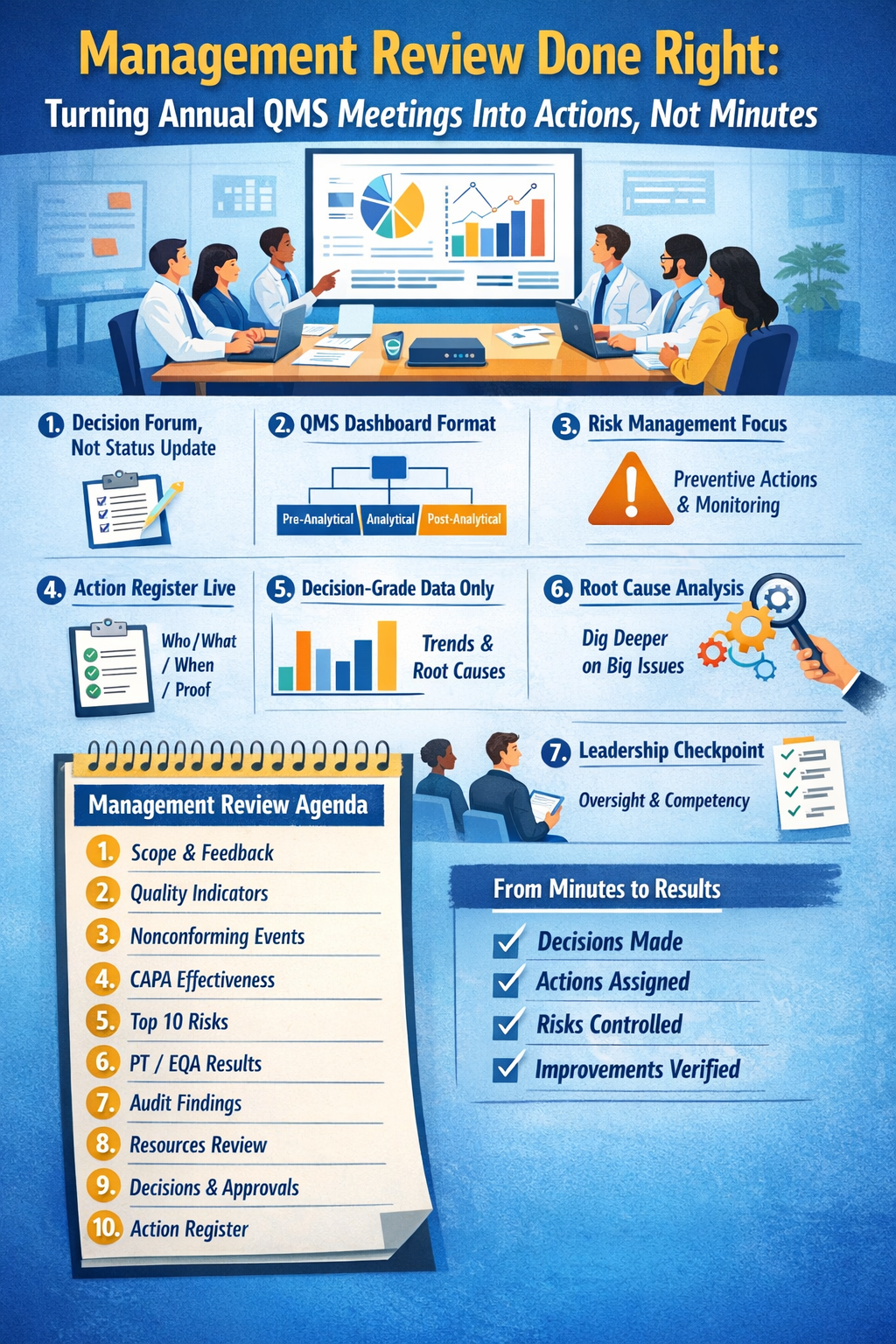
Turning annual QMS meetings into actions; not minutes
Most laboratories do hold an annual QMS/management review. The problem is what happens next: beautifully formatted minutes… and the same risks, the same repeat findings, and the same “we will monitor” statements that never become work.
A management review should function like your lab’s control room: one meeting where leadership decideswhat will change, assigns owners, allocates resources, and tracks effectiveness. That is exactly what a mature QMS expects evidence of monitoring, corrective action, risk management, and leadership oversight.
Below is a practical way to run a management review that inspectors recognize immediately because it produces traceable outcomes.
1) Redefine the meeting: it’s a decision forum, not a reporting session
If your meeting is mostly slides and “FYI updates,” it’s not management review, it’s a status call.
A good annual management review has three outputs only:
- Decisions (what we will change)
- Resources (people/time/budget/tools)
- Accountability (owner + due date + effectiveness check)
Everything else is input.
This aligns with how quality systems are evaluated in laboratory accreditation: monitor performance, identify nonconformities, take corrective/preventive action, and evaluate effectiveness.
2) Use a “QMS dashboard” structure that matches the lab workflow
Instead of organizing your agenda by departments, organize it by the end-to-end testing pathway:
A. Scope of service & customer needs
- Any changes in test menu, volumes, TAT expectations, service hours, referral patterns
- Complaints, satisfaction feedback, clinician concerns
A scope-of-service view is a recurring expectation: what services you provide, how you support users, and how you communicate performance.
B. Pre-analytical performance
- Specimen acceptance/rejection trends
- Patient/specimen identification errors
- Collection/transport issues, chain-of-custody (if applicable)
C. Analytical performance
- IQC trends & shifts
- Instrument downtime impact
- Method verification/validation summary (what changed this year)
D. Post-analytical performance
- Corrected reports trends
- Critical result notification performance
- TAT outliers and root causes
CAP explicitly expects quality indicators across pre-, analytic, and post-analytic phases, compared against defined targets.
3) Make risk management a standing item (not a last slide)
Most labs discuss risks only after something goes wrong. Mature systems run prospective risk management: what could go wrong, where, and what controls we will implement and monitor.
A simple way to do this in the meeting
For each top risk, force the discussion into five fields:
- Risk statement (cause → event → impact)
- Current controls (what already prevents/detects it)
- Gap (what’s missing or weak)
- Action plan (control improvement)
- Monitoring (what KPI or audit proves risk reduction)
If you do only one improvement to your management review, do this one: tie every “risk” to a measurable control and a monitoring plan.
4) Bring only “decision-grade” evidence (not raw data)
Leadership shouldn’t read 40 pages of logs. Bring decision-grade summaries:
- Trends (12 months)
- Thresholds/targets
- Outliers and causes
- Proposed actions with options (A/B) and impact
This is consistent with how QMS performance is assessed: indicators, nonconforming events, CAPA effectiveness not “data for data’s sake.”
5) Convert the minutes into an “Action Register” on the spot
Here’s the common failure mode: minutes are written after the meeting by one person, and “actions” become vague.
Fix: build the Action Register live during the meeting and display it while decisions are made.
Minimum columns that make inspectors happy
- Decision / action (specific and measurable)
- Owner (named person, not a department)
- Due date
- Resources needed (budget / headcount / IT / vendor)
- Evidence of completion (document, record, KPI)
- Effectiveness check (what will prove it worked, and when)
Why this works: QMS requires not only corrective/preventive actions, but also effectiveness evaluation.
6) Demand root cause logic for high-impact problems (and define “high-impact”)
If you treat all issues the same, you end up with shallow “retraining” fixes.
Set a rule in your QMS: events with patient potential harm, repeated events, or regulatory impact require deeper investigation and risk-based action. CAP explicitly expects RCA for sentinel-level events and a defined process to determine investigation depth for other risks/near misses.
7) Don’t skip the Director/Leadership effectiveness discussion
Annual management review is also a leadership effectiveness checkpoint:
- Are we adequately staffed and competent for the scope?
- Are delegations clear and working?
- Are recurring problems indicating weak oversight?
CAP’s Director Assessment emphasis is clear: systemic problems can reflect lack of effective oversight and governance.
EIAC similarly expects defined responsibilities, delegation coverage, and risk management as part of laboratory governance.
8) Include “facility & environment” only where it affects risk and flow
Environment discussions become useful when linked to risk and workflow: specimen reception flow, controlled access, safe pathways, temperature/humidity controlled storage areas, etc. Facility design and functional zones matter because they influence errors and safety.
Don’t present facility details as a tour—present them as risk controls.
9) A one-page agenda that works
Management Review Agenda (Annual)
- Scope of service changes + customer feedback (complaints/satisfaction)
- Quality indicators (pre / analytic / post) vs targets (trend + exceptions)
- Nonconforming events summary (themes, severity, recurrence)
- CAPA status + effectiveness results (what worked / didn’t)
- Risk register: top 10 risks + control performance + new risks
- PT/EQA & QC performance summary (including ungraded/late issues if any)
- Audit/inspection outcomes (internal + external) and repeat findings
- Resource review: staffing, training/competency, IT, equipment reliability
- Decisions & approvals: policies, objectives, major changes
- Action Register approval (owners, due dates, effectiveness plans)
- Include all relevant “periodic review” item in the Management Review agenda, as required by applicable accreditation checklists (e.g., scheduled review of policies, processes, and QMS performance).
This agenda maps cleanly to the expectations around QMS indicators, risk management, nonconforming event handling, and CAPA effectiveness.
10) What “good” evidence looks like during an inspection
When an assessor asks, “Show me management review,” the strongest evidence pack includes:
- Meeting agenda + attendance (with leadership participation)
- Pre-read dashboard (KPIs, risks, CAPA effectiveness, audit outcomes)
- Approved Action Register with owners/dates
- Follow-up evidence: closures + effectiveness checks completed
- Examples where management review triggered resourcing or policy change
That last point is the difference between a meeting and management review.
Thought: Annual QMS review is not a compliance ritual; it’s your lab’s yearly opportunity to reset priorities, remove barriers, and prove control. If you run it like a decision forum and track it like a project, you’ll stop producing minutes and start producing results.